
Flashback to the past a little bit with a post about it and a change of topic.
After I changed streams to a Psychology honors from a master’s in joint source coding and predictive variable modeling, I did a thesis in behavior modification under the best professor in the province. My supervising professor was the founding father of the research facility for behavioral intervention programs in St. Amant Hospital in Winnipeg, which was the only large-scale residential hospital for individuals with birth disabilities like chromosomal disorders and developmental disorders such as autism, mental retardation, et al. Research went sideways on devising different ways to help these individuals adapt to life.
A lot of people like to believe Psychology is all about Freud, Jung and all the general “talking stuff”. It is – if you want to take it lightly and it is NOT if you want to take it seriously. If you want to be the best in something – and I had a general rule that I would only work under the best, learn from the best and possibly be taught by the person who developed and founded the technique itself. If Aaron T. Beck founded cognitive behavioral therapy, then it is always worth it to attend a talk at the University of Pennsylvania by Aaron T. Beck. You never want to compromise on the teacher if you want to be the best with ludicrous thought processes in a field, and you want to be “moldable” enough for the teacher to work you up as they like.
However, since psychology was NOT the only program I had committed to, I DO NOT give the credit of my understanding of the subject to it.
Before Psychology, I was enrolled in a course which was a master’s in Joint Source Coding. This course was all about predictive variables and signal processing. Advanced, statistical, and digital signal processing were core to it. In short, random variables and how they intermingle and how you predict an outcome of a system. How do you predict the solution to a three-dimensional cube? Algorithms for pattern recognition schemas and fractals. The word “Predict” was pretty central to everything. Every single thing in the course had one requirement – random variables and probability. If one did not know these things, then one could not learn anything else from the course. Although I had minimal interest in the long-term future and engagement with the outcome of the course, as I did not see myself doing it for the rest of my life, I put in extra effort for one of the courses which drenched me and made me cry and also gave me sleepless nights, but yet became the focal point of the lens I used to deal with every other subject in the future. A course called “Pattern Recognition.”
The course was taught by a Polish professor named Miroslow Powlock, nicknamed “Mirek.” If you have seen the Oscar-winning movie “A Beautiful Mind,” with Russell Crowe portraying John Nash, the mathematician, then it is worth knowing that “Mirek” had a lengthy career working under the actual protagonist of the movie – the real John Nash. Mirek liked to go skiing, play with cubes in his office and find their solutions, and he had a dark sense of humor. “Mirek” also qualified as one of the top 2% scientists in the world. The course was built and designed to push you and to give you sleepless nights, the kind where you learn something new and your brain exerts extra pressure to create a framework for navigation, but once you get there, your brain does not go back to the old patterns of behavior.
From predicting the outcome of a system, I came into psychology. Sounds pretty different? Not if you enter the domain of behavior modification and prediction. A certain strain on the word prediction again.
Up there again in the department of psychology, I got some experience with the best – the director of the department of clinical psychology and pathology. The man had 30+ years of experience with psychopathological, delinquent, and antisocial elements, and he ran the entire department of clinical psychology and research under his belt. While working under him, it was imperative to be “moldable.” Since psychology is not a subject that one engages in behind the computer system and plays with cubes and their solutions – there was a tactile art and a “mindset” to it which you had to ruthlessly perfect. The director had an absolute loathing for the use of over-emotionality and sentimentality in the field while dealing with pathological clients. For the most traumatized individuals, there was an act of humanized empathy, but never any real involvement. After all, 30+ years of pathology, would you think he involved himself with everybody? The Director taught me a few things. When you meet pathology, you remain in observation mode, anecdotal to a bald eagle flying high above the ground with a sharp eye. The eagle observes, but nothing ever touches the eagle.

You never involve yourself with the client, and as you observe, you make mental notes and use your concrete knowledge to diagnose and offer treatment and intervention. The idea was that helping a client was impossible if there was any involvement with the client on any level at all. This approach made clinicians immune and almost inertly ruthless. Nobody understands how inertly cold the best psychologists and psychiatrists in the world actually are. You get their time, empathy, and understanding, but you will never know if it was genuine or if there was a real association behind it. The truth of the matter is, if you did get some “genuine” empathy or so, then either it was an act, or the clinician was not a great clinician.
The technique taught by the Director, Harold Wallbridge, which I developed and worked on, meant that I remained immune to almost all forms of vicarious trauma in my career. Many people asked me if my job “affected” me in any way – the answer was NO, and absolutely NOT. My job was FUN, and it was just a job, and I never came home with the burden of my work, and I never went to bed sleepless over a client. That’s what it means, doesn’t it – to learn from the best?
Moving on to behavior modification and prediction – again I was working with the best, my own supervising professor. The man taught me everything I needed to know about it. However, the real concreteness of thought behind it came from “Mirek.” Who said not completing a degree was a waste? It was never a waste if one single course could change you.
I told my professor I was not comfortable working with the population in St. Amanté and wanted to spread my wings a bit and experiment with different populations with different sets of challenges. I was redirected to a job at a provincial ward for level 5 delinquent youths—the worst in the province—funded by the federal government. Excited for my new work as a newbie behavior analyst, I couldn’t wait to apply everything I had learned to a different, more “challenging” set of population. The job was to create behavioral intervention strategies for harm reduction and recidivism in the population in the ward and to come up with quick strategies that the battered staff could apply to the inmates. What I did not expect was that the set of population was so challenging that it rendered me effectively useless…..
But i cant do anything with the “software” if the “hardware” is corrupt….
It is imperative to note that I had a strong grasp of behavior modification, but that was only a part of my honors thesis and was not the only thing I worked with. I was also versed in the structure of the brain, behavioral genetics – (again studying from the best professor in town who bred 12 dogs to determine if genetics impacted behaviors with lab rats for experimentation), a bit of pharmacology, and could read CT scans and PET scans of patient brains. It is important to understand that “talk therapy” or behavior modification techniques in delinquents go only as far as the brain is unafflicted. Experience has taught me that if the behavior was so unpredictable, and so off the beaten path, and there was a historical element of pathology or injury through a parent, then before applying the principles of behavior modification, it was imperative that we recommend the ward to a PET scan to get a scan of the brain and see what is really going on… Maybe we are just past the point?
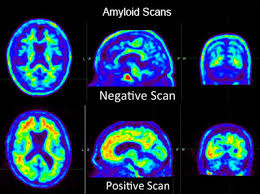
A PET scan is a machine where a harmless radioactive substance is injected into the bloodstream and, as the individual enters the scanner, the areas of the brain that are functioning and not functioning light up like a firefly under a microscope. This is particularly useful to assess which area of the brain is functional and which is not, and to determine if there are any birth defects in the brain that would bypass our ability to modify overt behavior. For those interested, a PET scan machine appears like an MRI machine, and the results tend to look a bit like this. A PET scan is so sophisticated that it can differentiate between a depressed brain and a manic brain.
Back to the Ward in question, a 15 year old female with an overly anti social behavior record, propensity to suicide, harming the staff on a regular basis and also self harming as a method for manipulation and Machiavellian. The ward being extremely violent and unworkable i began to suspect that this was not an ideal candidate for a behavior modification program and the current premise was not adequate to meet her needs. In Essence the ward was becoming a threat to the staff’s safety and i started suspecting if the province was looking at a legal lawsuit in the future. I will leave the sensational theatrics out of the description , however lets just say that level 5 youths are not individuals you will encounter on your regular sunny day outside your home….
For five days in a row I observed the female, made multiple notes, looked at her history and how she was born and in what circumstances she was born. It was evident that she was brought to the facility after birth immediately, given up for adoption, and her mother had delivered her in circumstances of heavy heroin addiction, likely having damaged her brain during gestation. Looking at all the information and after gathering everything, I decided that a behavior modification program was a waste of time before we determined what her brain actually looked like and if the parts of the brain that assisted in cognition and modularity were intact. I recommended her for a PET scan to see what was going on “inside her head” – literally.
Needless to say, the results came back and, as always, clinicians are strangely ecstatic to look at PET scan results because it is such a window into a person’s soul.
The results of the PET scan were so MIND-BLOWING that I took one look at it, dropped the report on the desk, and just sat back in shock as to how ANY human being could function with a brain like THAT, and still eat, sleep, and go about their random day. I was now not even a bit surprised at the violence the staff was encountering.
To elaborate – The ventricle tubules in her brain had actual holes in them. For the unversed, ventricle tubules are two moist tube-like structures which elongate from the spine and the nervous system and right up to the brain, spreading into the two hemispheres of the brain. The tubules carry a liquid substance inside them called cerebrospinal fluid, which is composed of ions, minerals, and many other things. The function of the tubules is to essentially “clean out” the brain as they take away debris back to the channel in the spine where the cerebrospinal column exists. The tubules carry a liquid and have a circulatory system involved, which is exactly why they say that “exercise is great for the brain.”
In essence the ventricle tubules look something like this in layman language.

Our wards’ ventricle tubules had holes in them, which meant that her cerebrospinal fluid was essentially seeping into both the hemispheres of her brain… This entire mayhem in her brain was ALL caused as a result of heavy heroin and alcohol use during pregnancy by her mother. Regardless, I was mind-blown to see the results of gestational alcohol and drug use on the brain of a little human being. It takes no effort to say that people who plan to have children should ward off any form of alcohol, cannabis, smoking, and any form of drug use, and this goes for the father involved as well.
I moved on to create a behavior prediction on the future behavior now, taking into account first hand the excessively violent behaviors of the ward. It became apparent, that the ward needed to be moved out of the facility into a locked psychiatric facility, preferably with sedatives and a locked jacket on. The timeline for a severe hostile behavior was less than 2 months at hand and alarm bells started ringing. In discussion with the supervisor of the facility a bit of an argument ensued about “the humane” element of moving a 15 yr old child into a locked psychiatric facility. I argued that it was what was “best for the child” considering that the behaviors were so violent that it had a high likelihood of producing a fatality or a casualty within the next 2 month window maximum and if not acted upon the likelihood of a slapstick lawsuit was evident.
I was asked – well, what good are YOU for? Aren’t YOU here for “modifying her behavior” and helping out in reducing essentially just “that”? The PROBABILITY of her causing a FATALITY?
But I can’t do anything with the “software” if the “hardware” is corrupt…. – I protested…….

Indeed such decisions are never easy, and the supervisor stormed off saying that she needed time to think and needed a second opinion. Within 30 minutes of the supervisor storming out, ……3….2….1…. the ward brought a rock from outside and sodomized a staff member on the face …..
Police were called right away, and the staff was taken away. The ward was immediately moved to a locked psychiatric facility – the one I had recommended. Was this luck? A hard sell.
After the ward was moved on the same day, the supervisor came to me, confused and sad but visibly and strangely impressed and taken aback, and asked, “So WHERE did you learn this strange behavior modification and prediction thing from exactly?” …..
……..

Leave a comment